Human skin is more than a protective layer; it is a living record of our lives, bearing the marks of sunlight, aging, and environmental exposure. Over time, normal signs of aging—freckles, wrinkles, and rough patches—accumulate, yet some changes signal more serious concerns. Actinic keratoses (AKs) are small, persistent, rough patches that develop primarily from ultraviolet (UV) damage to skin cells’ DNA. These lesions are precancerous and can evolve into squamous cell carcinoma if left untreated. Often subtle and painless, they are most common in adults over fifty, whose skin has endured decades of sun exposure. Recognizing them early is a powerful preventative measure, offering the opportunity to intervene before progression to cancer and emphasizing that cumulative sun exposure, even when unnoticed, has tangible consequences.
The development of actinic keratoses begins with ultraviolet radiation—both UVA and UVB—from sunlight, which penetrates skin layers and can damage the DNA of cells responsible for maintaining the skin’s barrier. While many damaged cells are repaired naturally, some persist and begin multiplying abnormally, forming rough, scaly patches. AKs appear primarily on sun-exposed areas such as the face, scalp, hands, forearms, ears, neck, and lower lips. They are typically flesh-colored, red, or brown, and range from flat to slightly raised, sometimes crusted. Though pain is uncommon, the persistence and texture of these lesions are key identifiers. Over time, untreated AKs carry roughly a ten percent chance of developing into squamous cell carcinoma. Given the millions of cases each year, this small individual risk translates into a significant public health concern, highlighting the need for awareness and vigilance.
Certain populations face higher risk for actinic keratoses. Fair-skinned individuals who burn easily or have light eyes and hair, outdoor workers such as farmers, lifeguards, and construction employees, and people living in high-UV regions are especially vulnerable. Immunocompromised individuals, including organ transplant recipients, are also prone to developing multiple lesions and may progress to skin cancer more rapidly due to weakened immune defenses. Repeated sun exposure over a lifetime can accumulate dozens of AKs alongside other sun-induced skin changes, such as liver spots, thinning skin, and wrinkles. At a cellular level, UV rays induce DNA mutations, and over time, abnormal cells multiply, eventually breaching the boundary between the epidermis and dermis and forming invasive squamous cell carcinoma. This slow progression underscores the importance of early detection as a means of prevention.
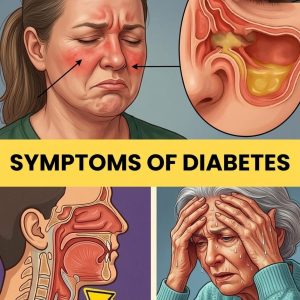
Early recognition of actinic keratoses is critical. Signs include rough, scaly patches that persist despite moisturizers, red or sunburned-appearing areas that do not heal, recurring crusts, and firm bumps that may be tender to touch. Texture is often more revealing than appearance, with lesions sometimes catching on fingernails or forming clusters on sun-exposed regions. Dermatologists diagnose AKs through visual inspection and dermatoscopic tools, confirming suspicious spots with biopsies when necessary. Treatments vary depending on severity and number of lesions. Cryotherapy freezes individual lesions quickly, while topical creams like 5-fluorouracil or imiquimod treat multiple areas. Photodynamic therapy uses light-sensitive medication to destroy abnormal tissue with minimal scarring, and thicker lesions may require curettage or laser treatment. With early intervention, most lesions resolve fully, often after a single treatment session.
While a diagnosis of “precancerous” can be alarming, dermatologists emphasize that identifying actinic keratoses presents a crucial opportunity for prevention. The diagnosis encourages protective behaviors: consistent sunscreen use, wearing hats and clothing that shield the skin, avoiding peak sun hours, and scheduling regular skin exams. Distinguishing AKs from benign spots like age spots or seborrheic keratoses requires training, as these commonly accompany aging. Age spots are smooth and flat; seborrheic keratoses appear waxy or “stuck on”; AKs are rough to touch. Misidentification or delayed evaluation can allow progression to squamous cell carcinoma, which is highly treatable when caught early but can penetrate deeper skin layers if ignored. Melanoma, though less commonly confused with AKs, remains the most dangerous form, presenting as dark, irregular moles with uneven borders and color. The shared characteristic of these cancers is persistence beyond the normal lifespan of skin cells.
Globally, cases of actinic keratosis are rising, linked to greater sun exposure, longer lifespans, and increased awareness. In the U.S., over fifty million people receive treatment annually, while in Australia, roughly half of adults over forty develop at least one AK. Advances in detection, including full-body skin checks, digital imaging, and mole-mapping software, have improved outcomes, while home-based monitoring tools allow individuals to track changes between professional visits. Stories of early intervention demonstrate the importance of vigilance, as minor lesions treated promptly prevent progression to cancer. With protective habits, routine exams, and timely treatment, people can continue to enjoy outdoor life safely. Human skin, resilient and capable of self-repair, provides guidance through its changes, and attentive care allows us to balance sun exposure with long-term health, ensuring that every patch, line, and mark serves as a message rather than a warning left unread.